What is Chronic Care Management?
CCM is the care coordination that is outside of the regular office visit for patients with multiple (two or more) chronic conditions expected to last at least 12 months or until the death of the patient, and that place the patient at significant risk of death, acute exacerbation or decompositions, or functional decline. It can be delivered to people with many
Components of Implementing CCM
Patient Consents & Initial Setup
Acquire consent from patient to provide CCM services (Verbal and written(Annually)
Establishing, Implementing, and Revising Care Plan
Provide comprehensive care plan for health management goals
Monitoring Data and Billing
Supply continuity of care thru care members and submit billing for reimbursement
The Workflow
Plan
Create a CCM work-flow, establish documentation, and CCM billing procedure
Train
Train qualified Physicians and clinical staff to provide monitoring services.
Consent
Acquire consent from the patient to be remotely monitored
Educate
Educate patients on how to measure oxygen and blood pressure health data using Connect+ to collect heath data
Sync
Patient health data sync automatically and is monitored by physicians/clinical staff.
Submit
Submit eligible patients for billing and get reimbursed for monthly monitoring.
CCM Pathway
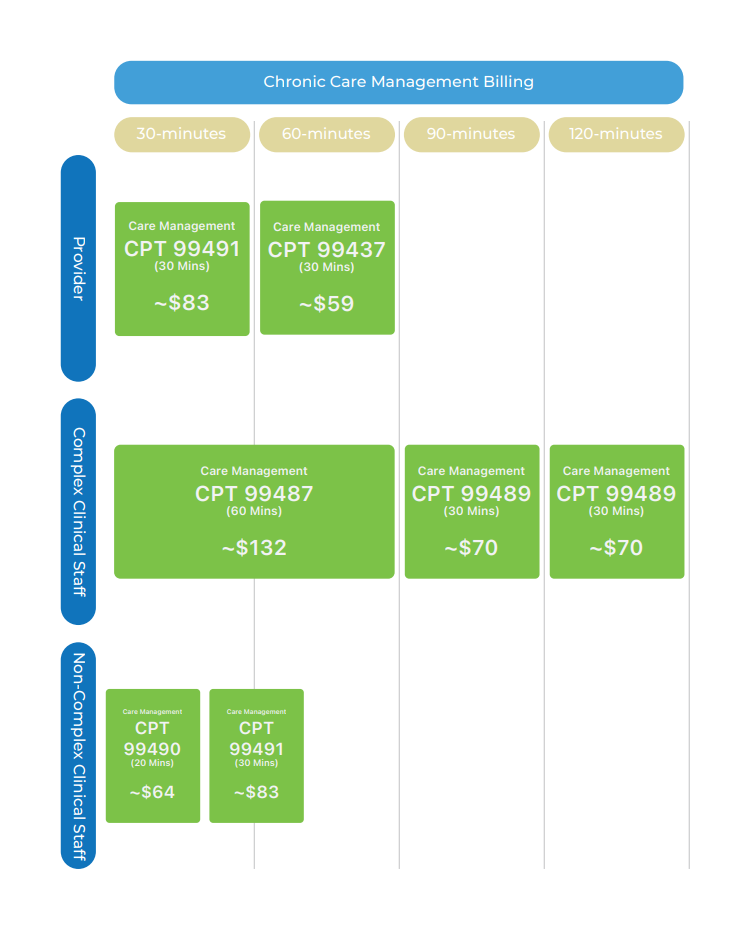
Non-Complex Chronic Care Management Billing Codes
CPT 99490
Initial Chronic Care Monitoring (Staff)-
Chronic care management services, at least 20 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month.
CPT 99439
Subsquent Chronic Care Monitoring (Clinical Staff)-
Chronic care management services, subsequent 20 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month.
CPT 99491
Initial Chronic Care Monitoring (Physician)-
Chronic care management services, provided personally by a physician or other qualified health care professional, at least 30 minutes of physician or other qualified health care professional time, per calendar month.
CPT 99437
Subsquent Chronic Care Monitoring (Physician)-
Chronic care management services, provided personally by a physician or other qualified health care professional, subsequent 30 minutes of physician or other qualified health care professional time, per calendar month.
Non-Complex Chronic Care Management Billing Codes
CPT 99487
Initial Chronic Care Monitoring (Staff)-
Chronic care management services, at least 60 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month.
CPT 99489
Subsquent Chronic Care Monitoring (Clinical Staff)-
Chronic care management services, subsequent 30 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month.
Frequently Ask Questions
The difference bewteen CCM vs Complex CCM?
There are two different types of CCM. Classic chronic care management and complex chronic care management. Standard CCM can be distinguished from complex CCM by the respective CPT code. Complex CCM uses codes 99487 and 99489. Complex CCM patients’ care teams must have a significant establishment or revision of the care plan and typically communicate more with the care team staff in a calendar month.
Which practitioners are eligible to bill Medicare for CCM?
Physicians (regardless of specialty), advanced practice registered nurses, physician assistants, clinical nurse specialists, certified nurse-midwives, or the provider to which such individual has reassigned his/her billing rights are eligible to bill Medicare for CCM. Other non-physician practitioners and limited-license practitioners (e.g., clinical psychologists, social workers) and providers not eligible for reimbursement under the Medicare Physician Fee Schedule (e.g., pharmacists) cannot bill for CCM.
Are there specific services the billing practitioner must furnish to a beneficiary as a prerequisite to providing CCM for that beneficiary?
If the billing practitioner has not seen the beneficiary in the last 12 months (or if the beneficiary is a new patient), the practitioner must discuss CCM with the beneficiary as part of a face-to-face visit (e.g., regular office visit, annual wellness visit [AWV], or initial preventive physical exam [IPPE]), prior to billing for CCM for that beneficiary. The face-to-face visit is not a component of the CCM service, and thus may be billed separately. An initiating visit is not required for the practitioner to begin billing for CCM services as long as he or she: (1) has beneficiary consent, and (2) has seen the patient within the last 12 months.
What type of consent is required?
The practitioner must document in the beneficiary’s medical record that the required information was provided and that the beneficiary explicitly accepted the services.
What items are typically included in a care plan?
According to CMS, a care plan should include the following:
- A problem list, expected outcome and prognosis, and measurable treatment goals
- Symptom management and planned interventions (including all recommended preventive care services)
- Interaction and coordination with outside resources and practitioners and providers
- Medication management (including a list of current medications and allergies, reconciliation with review of adherence and potential interactions, and oversight of patient self-management)
- Responsible individual for each intervention
- Requirements for periodic review/revision
When filing a claim for CCM, what should be listed as the date of service?
The billing practitioner may list as the date of service the day on which the 20-minute minimum requirement is satisfied or any day thereafter through the end of the calendar month. If the beneficiary dies during the month, the claim for CCM will be paid only if the date of service is prior to the date of death.
What should be listed as the place of service?
The billing practitioner must list as the place of service the location at which he or she would furnish a face-to-face office visit with the beneficiary. Thus, a practitioner who practices in a hospital outpatient department must list "2" as the place of service on the CCM claim form, triggering payment at the facility rate.